Peripheral arterial disease (PAD) i.e. disease of arteries of the peripheries, is often an unrecognized manifestation of atherosclerosis and other vascular disorders. The disease prevalence is in the range of 3% to 10%, increasing to 15% to 20% in persons over 70 years.
The classic symptom of PAD is intermittent claudication (IC). It is usually diagnosed by a history of leg pain on exercise that is relieved by a short rest. However most of the patients of PAD tend to be asymptomatic or have muscular symptoms that are not typical of IC. Critical limb ischemia (CLI) is the most severe manifestation of PAD. The blood supply is inadequate to meet the demands of the tissues even at rest, hence patients tend to have pain at rest and / or tissue loss with difficulty in healing.

Based on epidemiological studies the individuals particularly at risk for PAD are
- Age less than 50 years with diabetes, and one additional risk factor (e.g. smoking, dyslipidemia, hypertension, or hyperhomocysteinemia)
- Age 50 to 69 years and history of smoking or diabetes
- Age 70 years and older
- Leg symptoms with exertion or ischemic rest pain
- Abnormal lower extremity pulse examination
- Known atherosclerotic coronary, carotid, or renal artery disease
Natural history of PAD is not determined by the severity of symptoms of IC, but by the extent of atherosclerosis in the limbs and elsewhere. The PAD patients have increased cardiovascular mortality as compared to healthy individuals. There is risk of progression of disease and limb amputation especially in the patients with critical limb ischemia. However most of the patients tend to have stability of symptoms over the period of time.
Evaluation of apatient of PAD essentially involves the examination of all the superficial arteries of the body. Any deficiency, asymmetry of pulsations or bruits are suggestive of PAD. Evidence of atherosclerosis elsewhere should also be looked for.
The diagnostic work-up of a patient of PAD typically involves measurement of Ankle-brachial index (ABI) at the initial visit.
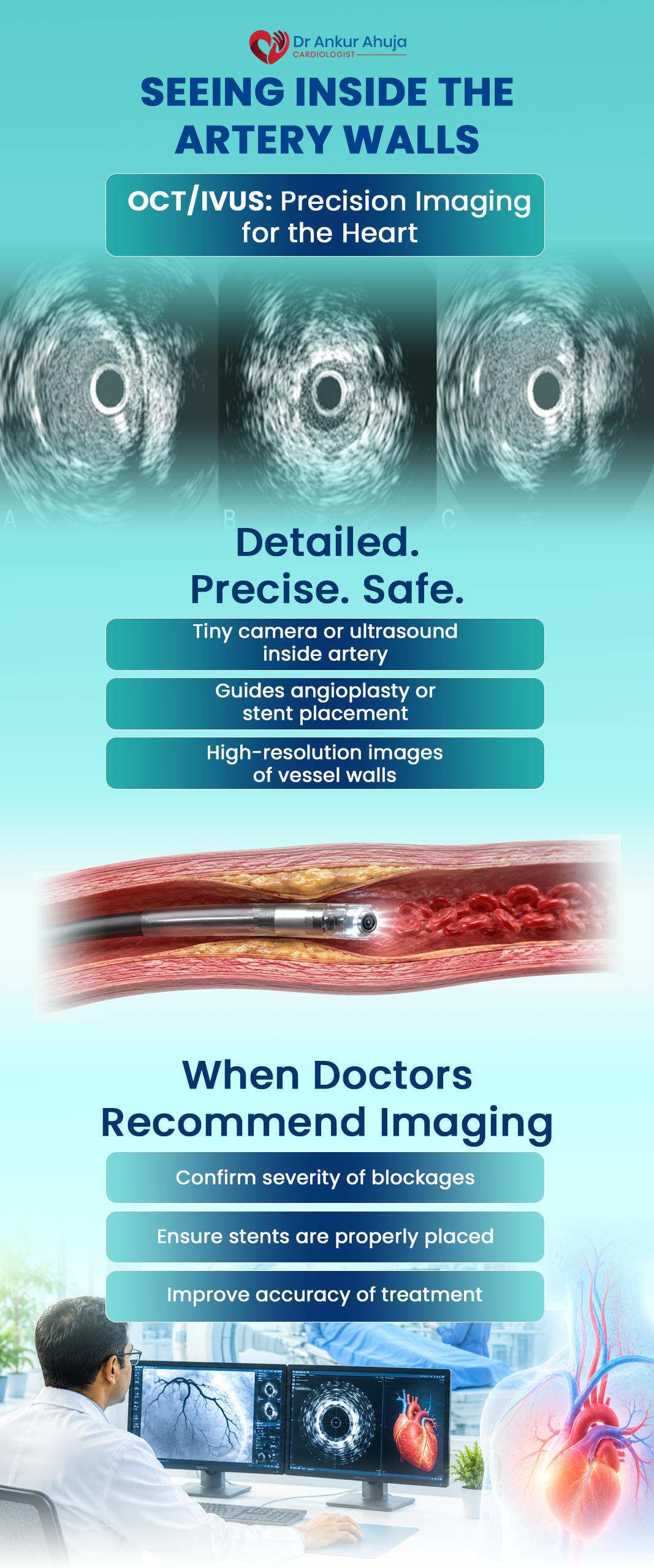
Other diagnostic tests for evaluation of PAD include exercise ABI, segmental pressures, pulse volume recordings, duplex ultrasonography, CT or MR angiography and conventional angiography.
Duplex ultrasonography is the most widely available and most often used test for initial assessment of the disease. CT or MR angiography give a more detailed and accurate picture; however they are costly and less easily available. Conventional angiography is the gold standard test for PAD, though it is now uncommonly used as a first line test.
Management of PAD involves three strategies-
- Management of risk factors
- Pharmacological management
- Invasive management
PAD being a manifestation of atherosclerosis just as in coronaries or elsewhere, requires management goals for its risk factors as for CAD.
Physical activity is an important part of the management of PAD as regular supervised training helps increase the claudication distance.
Symptomatic treatment of the disease is best done by phosphodiesterase III inhibitor cilostazol given in doses upto 100mg twice a day. It should be avoided in heart failure patients. Importantly statins have also been shown to improve claudication distance. Pentoxifylline though long used, has not shown consistent benefits in IC patients. Angiogenic growth factors have also been evaluated, however they are still to show the benefit in clinical trials.
Interventional therapy has also come to play a major part in the management of IC. Surgical therapy used to be the first choice in all patients in yesteryears. However with the ever increasing availability and vastly improving results ofangioplasty, it has now replaced surgery in most of the patient subgroups as only/initial interventional therapy. The indications include-
- Incapacitating claudication
- Limb-threatening ischemia (pain at rest, non-healing ulcers and/or infections or gangrene)
- If symptoms persist despite medical therapy and patient has inflow disease amenable to angioplasty with low risk
To conclude, PAD as a disease entity is often under-diagnosed and consequently under-treated. Increasing levels of awareness are required to manage this problem. A lot of scientific research is still underway in the search for adequate medical and interventional management of these patients.